
Clinical Pathology
HOME > Activities > Clinical Medicine > Clinical Pathology
1.Research Summary
In the field of clinical pathology, we conduct research mainly on digestive organ pathology using human tissues. We proceed with this research by adding immunohistological and molecular biological techniques to morphological analysis.
2.Organs used for research
- Large intestine
- Stomach
- Esophagus
- Liver, gallbladder and pancreas
3-1.Research subjects of the large intestine
- Pathological features of inflammatory carcinogenic lesions and carcinogenic mechanism
- Domestic collaborative research on cancer surveillance of ulcerative colitis
- Development and patterns of growth and extension of colorectal cancer tissues and underlying molecular mechanisms
- Diagnosis of malignant grade of colorectal cancers
3-2.Research subjects of the stomach
- Histopathological analysis of early gastric cancers after pylori eradication
- Investigation of the expressions of characters in gastric-type adenocarcinomas
- Expression of AMACR in gastric adenocarcinomas
- Expression of AMACR in gastric endocrine tumors
- Expression of mucus phenotype in gastric endocrine tumors
- Comparison of NBI and construction of 3D images of pathological tissues in early gastric cancers
3-3.Research subjects of the esophagus
- Histopathological and molecular pathological analysis of intramucosal squamous cell tumors of the esophagus
- p53 gene mutations in the early lesions of esophageal squamous cell carcinomas
- Histological features and mucus phenotype of the mucosa at the esophagogastric junction
- Development and extension of Barrett’s esophagus
- Distribution of mucus phenotype in Barrett’s esophageal adenocarcinomas
3-4.Liver, gallbladder and pancreas research subjects
- Intrahepatic extension patterns of hepatocellular carcinomas
- Development of tissues and growth and extension patterns of biliary carcinomas
- International collaborative research on gene abnormalities involved in the development of gallbladder cancers
4.Research Results
|
[Area] Clinical pathology (large intestine) |
|
|
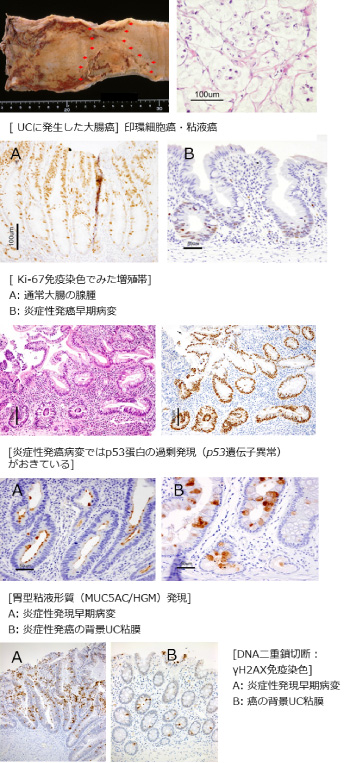
[Research subject] Pathological features of inflammatory carcinogenic lesions and carcinogenic mechanism |
|
|
[Description] |
[Photographs]
|
|
[Area] Clinical pathology (stomach) |
|
|
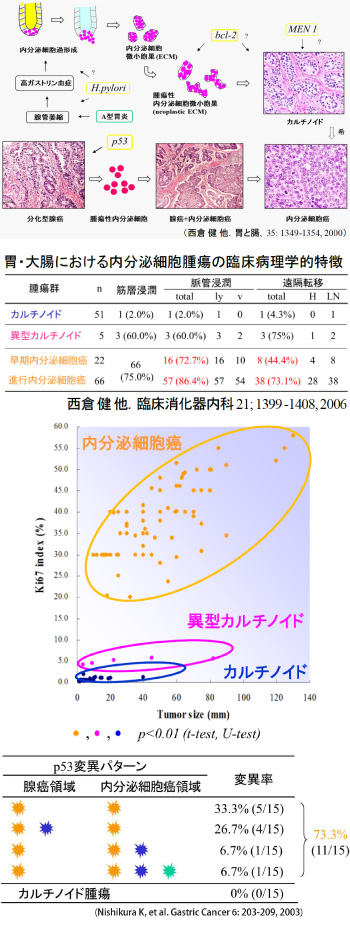
[Research subject] Gastrointestinal endocrine tumors |
|
|
[Description] |
[Figures and Tables]
|
|
[Area] Clinical pathology (Esophagus) |
|
|
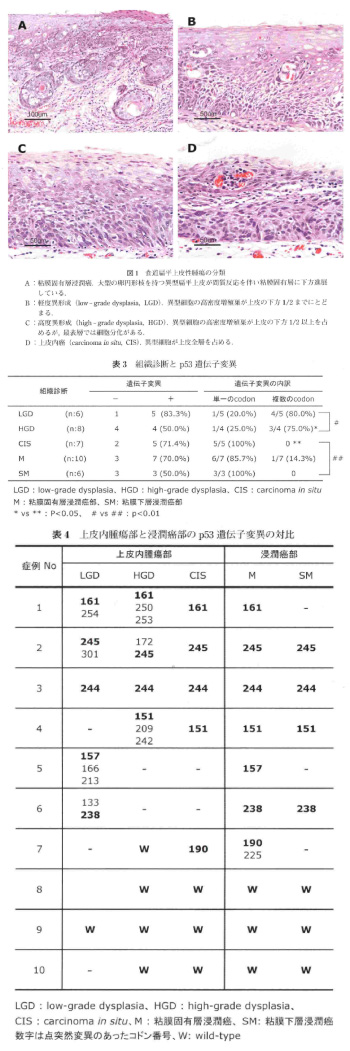
[Research subject] p53 gene mutations in the early lesions of esophageal squamous cell carcinomas |
|
|
[Description] |
[Figures and Tables] |
Please see the Clinical Pathology website for a detailed description of our research.