|
|
|
|
|
|
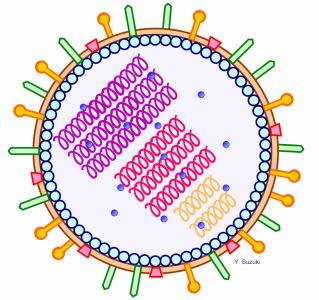
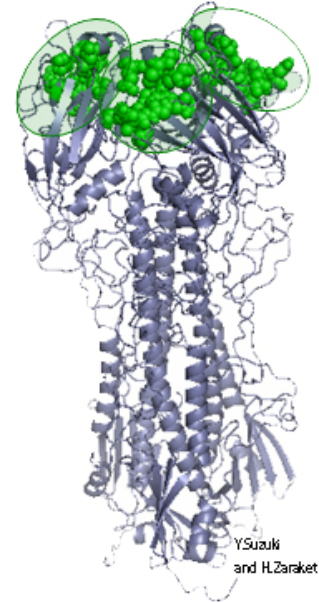
インフルエンザは温帯では冬に流行りますが、熱帯ではいつ流行るのかわかっていない場合が多いです。最近、熱帯・亜熱帯で雨期にインフルエンザが流行りやすいことが分かってきました。当教室では、過去にベトナム、ミャンマーでインフルエンザの疫学調査を行い、雨期に流行ることを明らかにしました。 インフルエンザは抗原変異を繰り返すために一生のうちで何回もインフルエンザに感染します。インフルエンザの大きな謎の1つは、どこで新しい株が生まれるかということです。最近の研究では新しい株はアジアで発生して世界中に広がることが多いと考えられています。当教室では、日本のインフルエンザと世界各地のインフルエンザの遺伝子を比較し、どのような経路でインフルエンザが伝播しているのか解明に取り組んでいます。 近年、インフルエンザ感染症に対して抗ウイルス薬で治療が可能となりました。日本で保険適応されているのはM2阻害剤のアマンタジンと、ノイラミニダーゼ阻害剤のオセルタミビル、ザナミビル、ペラミビル、ラニナミビルです。M2阻害剤はA型インフルエンザにのみ有効ですが、ノイラミニダーゼ阻害剤はA型、B型インフルエンザ双方に有効です。症状がでてから48時間以内に治療を開始すれば、有熱期間が1-2日短縮されます。抗インフルエンザ剤は治療後に耐性が出現することが知られています。M2阻害剤では治療後の約1/3に、ノイラミニダーゼ阻害剤のオセルタミビルではA/H1N1の約1割に耐性が出現します。一般的に耐性株は伝播力が弱いとされており、これまで耐性株が流行することはないと考えられてきました。しかし、2005年にアジアを中心にアマンタジン耐性A型が大流行し、2007年にはヨーロッパに端を発したオセルタミビル耐性A/H1N1株が世界中で流行しました。幸い、インフルエンザA/H1N1 2009(新型インフルエンザ)に耐性株の流行はまだありません。 当教室では、インフルエンザの分子疫学と薬剤耐性に焦点をあてて研究を行っています。これまで日本のみならずミャンマー、ベトナム、レバノン、極東ロシアなどでインフルエンザの調査を行ってきました。ミャンマーでは世界的に珍しいザナミビルとアマンタジンの二重耐性A/H3N2を検出し英文誌に報告しました。(Dapat et al., EID 2010) 新潟大学ではインフルエンザの検出だけでなく海外のインフルエンザ研究室の技術支援を積極的に行ってきました。ベトナム、ミャンマーでは国立研究所のインフルエンザ・ラボの支援と整備を行い、これらの研究室がWHOのナショナル・インフルエンザ・センターに認定されるために大きく貢献をしました。 Influenza causes epidemic during winter time in temperate countries, but limited information is available on circulation of influenza in tropical areas. Previous studies show in tropics influenza is detected throughout year, but outbreaks are likely to occur during rainy season. We have clarified seasonality of influenza in North Vietnam and Myanmar where information was limied. Another question remains with influenza is where new strains of influenza occur in the world. Most recently, a source-sink model of influenza virus evolution has been proposed, whereby new virus variants preferentially emerge out of the tropics, in particular from East-SouthEast Asia, and seed epidemics in temperate areas. One of our purposes is to Other focus is antiviral resistance of influenza. Currently, two types of anti-influenza drug are in clinical use in Japan, M2 inhibitors (amantadine) and neuraminidase inhibitors (oseltamivir, zanamivir, peramivir, laninamivir). M2 inhibitors are effective for influenza A, but neuraminidase inhibitors are effective for both influenza A and B. Both drugs can reduce illness days by 1- 2 days when they are administered within 48 hours of symptom onset. It is reported that one third of influenza patients can develop resistance after treatment by M2 inhibitors and 10% by one of neuraminidase inhibitors, oseltamivir. Viral resistance is derived from point mutation at functional protein (M2 protein or neuraminidase), and in general, fitness at the time of human to human transmission is reduced with resistant strains compared to wild strains. Thus it was believed resistant strains do not increase in the community. However, in 2005 amantadine resistant influenza A showed a dramatic rise in community circulating strains without pressure of the M2 inhibitors and then in 2007, oseltamivir resistant influenza A/H1N1 (seasonal) caused epidemic firstly in Europe and spread to the rest of the world. Thus, picture for drug resistant influenza strains are changing in recent years. So far, there is no increase of oseltamivir resistant strains in A/H1N1 pdm in the community. Niigata University is one of National Universities in Japan located North West of Japan main island, and working on influenza viral surveillance. We are focusing on molecular epidemiology and anti-viral resistance of influenza. In the past, we investigated influenza not only in Japan but various countries such as Myanmar, Vietnam, Lebanon and Far East Russia, which is regarded as hot spot in influenza dynamics. We found rare double resistant strains for zanamivir and amantadine in influenza A/H3N2 in 2007 and 2008 in Myanmar and reported to international English journal (Dapat et al., EID 2010). Niigata University is not only working on analyses of influenza, but has ability to upgrade influenza laboratory for molecular diagnostics. We worked with national laboratories in Vietnam and Myanmar, and the two laboratories were designated as National Influenza Center in WHO Global Influenza Surveillance Network. |
|
||||||||||


Copyright(C)2011 Division of International Health, Niigata University All Rights Reserved.