![]()
![]()
1.Research Summary
In the field of clinical pathology, we conduct research mainly on digestive organ pathology using human tissues. We proceed with this research by adding immunohistological and molecular biological techniques to morphological analysis.
2.Organs used for research
3-1.Research subjects of the large intestine
3-2.Research subjects of the stomach
3-3.Research subjects of the esophagus
3-4.Liver, gallbladder and pancreas research subjects
4.Research Results
[Area] Clinical pathology (large intestine)
[Research subject]
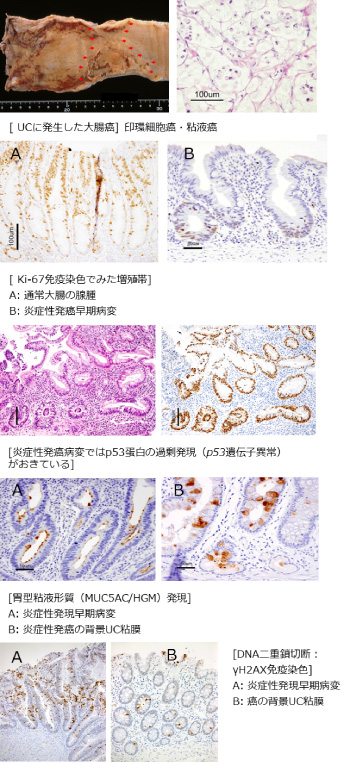
Pathological features of inflammatory carcinogenic lesions and carcinogenic mechanism
[Description]
In long-term inflammatory bowel diseases (ulcerative colitis (UC) and Crohn’s
disease), colorectal cancers occur more commonly, and this is referred
to as inflammatory carcinogenesis. In our department, we conduct research
on pathological features and carcinogenic mechanisms of early carcinogenic
lesions mainly of UC and have clarified the following points:
In recent years, the frequency of inflammatory bowel diseases has also been increasing in Japan. With this, cases suffering from long-term inflammatory bowel diseases have been increasing in number, and this necessitates the development of biomarkers for the early detection and precise pathological diagnosis of inflammatory carcinogenic lesions. This research is also important for addressing these clinical needs.
[Photographs]
[Area] Clinical pathology (stomach)
[Research subject]
Gastrointestinal endocrine tumors
[Description]
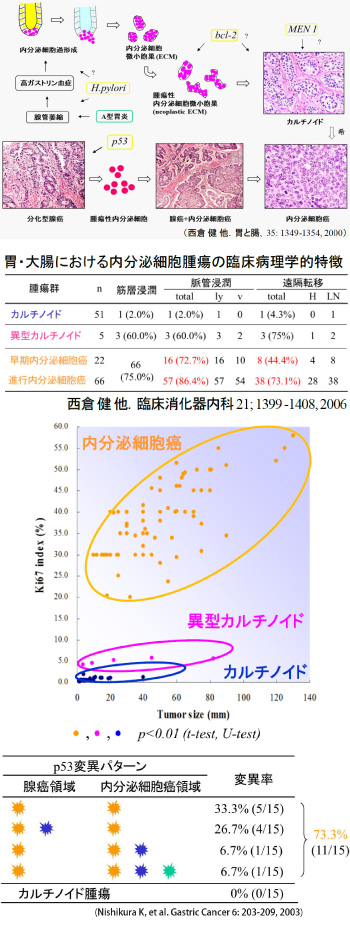
Endocrine tumors which develop in the gastrointestinal tract are broadly
divided into carcinoids and endocrine cell carcinomas. They differ not
only in morphology and biological malignancy but also in histogenesis.
[Nishikura K, et al., The stomach and intestines 35: 1349-1354, 2000]
Most carcinoids do not progress to muscle invasion or metastases, but endocrine
cell carcinomas develop metastases at high rates from the early stage.
In addition, among various tumors (carcinoids, atypical carcinoids and
endocrine cell carcinomas), cellular proliferative potentials differ significantly
(carcinoids < atypical carcinoids ≪ endocrine cell carcinomas). [Nishikura
K, et al., Clinical Gastroenterology 21; 1399 -1408, 2006]
Histogenesis of carcinoids (cases with type A gastritis): Hypergastrinemia
occurs secondary to reduced gastric acid secretion associated with fundic
gland atrophy, endocrine cell hyperplasia within the affected crypts occurs
(via the trophic action of gastrin), and, furthermore, the ECM is formed
outside of the duct, which becomes a tumor leading to carcinoid formation.
[Itsuno M, et al. Cancer 63: 881-890, 1989]
Histogenesis of endocrine cell carcinomas: A transition from carcinoids
is rare, and endocrine cell carcinomas occur with preceding neoplastic
endocrine cells with the adenocarcinomas as the site of origin. The bases
for this are as follows:
[Figures and Tables]
[Area] Clinical pathology (Esophagus)
[Research subject]
p53 gene mutations in the early lesions of esophageal squamous cell carcinomas
[Description]
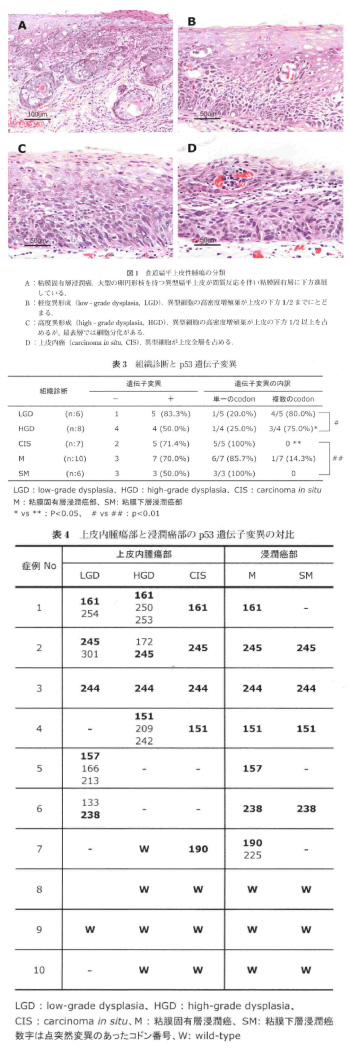
In esophageal squamous cell carcinoma, precancerous lesions are atypical
squamous cells collectively referred to as showing the features of dysplasia,
which are considered to progress to invasive carcinomas through the process
of carcinoma in situ (CIS). Dysplasia is broadly divided into low-grade
dysplasia (LGD) and high-grade dysplasia (HGD), but it is not clear which
of the two is an early carcinogenic stage for the esophageal squamous epithelium.
In order to clarify the above, we focused on the p53 gene abnormalities
frequently observed in esophageal squamous cell carcinomas, and investigated
p53 gene mutations in squamous cell carcinomas and comorbid tumors in situ
(LGD, HGD and CIS) as well as p53 protein overexpression. In 10 patients
who underwent endoscopic resection for esophageal squamous cell carcinomas
(invasive carcinoma in the lamina propria: M carcinoma in 4 patients, invasive
carcinoma in the submucosal layer: SM carcinoma in 6 patients), we evaluated
p53 immunostaining at sites of LGD, HGD, CIS, M carcinoma and SM carcinoma,
and searched for p53 gene mutations. p53 gene mutations were observed in
83% of LGD, 50% of HGD, 71% of CIS, and 50%-75% of invasive carcinoma sites.
In LGD and HGD, mutant codons were shared by CIS and invasive carcinoma
sites coexisting in the same lesions except in one case, or both were wild
type. From the above, it was estimated that LGD and HGD showed histogenetic
continuity with CIS and invasive carcinoma sites in the same lesions. Gene
abnormalities occurred in a single mutant codon in CIS and invasive carcinoma
sites in the same lesions, but diversity was observed in mutant codons
in LGD and HGD (there were multiple mutant codons). LGD and HGD were considered
to consist of multiple cell populations with different p53 gene mutations,
which become CIS with a uniform p53 gene mutation pattern through clone
selection and then invade the lamina propria of the mucous membrane. From
the results of this research, it was estimated that cell populations, in
which p53 gene mutations common to both CIS and invasive carcinomas have
already occurred, are already included in the LGD stage and that LGD can
be positioned as an early carcinogenetic stage of the esophageal squamous
epithelium. Therefore, an active clinical approach is considered to be
required for LGD. [Tsuboi K. Niigata Medical Journal 124: 627-637, 2010]
[Figures and Tables]
Please see the Clinical Pathology website for a detailed description of our research.