![]()
![]()
1.Research Summary
Urology is a field of medical care in which various diseases of the adrenal gland, kidney, urinary tract, and male genitalia are diagnosed and studied by taking advantage of surgical and medical methods (see website of the Japanese Urological Association).The Department of Urology is divided into the Urological Oncology Group, Male Function Group, Kidney Transplantation Group, and Urinary Physiology Group, and is currently conducting intensive research on kidney transplantation and urological oncology.
2.Research Groups
3-1.Kidney Transplantation Group
Research subjects
(Kaken A, Kaken C)
Since the shortage of organ transplants has become a worldwide problem,
We have successfully performed the first ABO-incompatible kidney transplantation
in January 1989 and spent tremendous efforts to advance this procedure
for more than a quarter century to date. To control acute antibody-associated
rejection caused by the recipient’s anti-A/B antibody against the donor
blood type, we have implemented various strategies since the beginning.
We reported that a new treatment strategy based on desensitization incorporating
rituximab, which controls B cells, yields good graft survival rates. Furthermore,
we discovered and reported that the ABO histo-blood type antigens expressed
on renal vascular endothelial cells were different from those on red blood
cells for the first time. Therefore, we have recently concluded that transplantation
could be successfully performed without removing anti-A/B antibodies even
if even if the recipient’s had relatively high antibody titer measured
by using red blood cells.
The induction mechanism of immunological accommodation that occurs after
ABO-incompatible kidney transplantation has not yet been elucidated, however,
we have thus been investigating this mechanism from various aspects, including
alteration of the antigenicity of ABO histo- blood group antigens, modulation
of host immunity, especially in antibody production by B cells and plasma
cells, and changes in complement regulation factors.
References
References
3-2.Urinary Oncology Group
Research subjects
Mechanism of androgen signals in prostate cancer cells
Collaborative research on BCG therapy for 2ndTUR-negative cases in pT1G3
bladder cancer (JCOG)
Collaborative research on the establishment of regions for lymph node dissection
in renal pelvic and ureter cancer (JCOG)
Prognosis and QOL after intensity-modulated radiation therapy and brachytherapy
for prostate cancer (collaborative research with the Department of Radiology)
Multicenter study of sorafenib and sunitinib administered by crossover
design for renal cell cancer.
Multicenter study on the optimal dosing interval of zoledronic acid for
cM1b prostate cancer.
4.Research results
[Area] Kidney transplantation
[Research subject]
ABO-incompatible renal transplantation
[Description]
We performed a comprehensive proteome analysis of proteins with ABO-type
antigens (antigenic carbohydrate) using proteins extracted from human renal
tissues. Subsequently, we confirmed that each antigen is expressed in human
kidneys and has ABO-type antigen and revealed that it is present in a manner
different from the proteins in red blood cells (Fig 1).
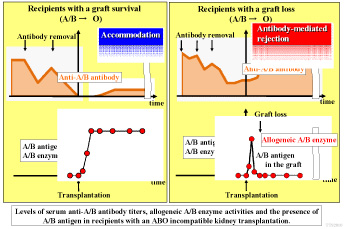
ABO-type antigen synthases are present in serum as well. We investigated
donor blood type synthases in the blood of donors after ABO-incompatible
kidney transplantation. We discovered that donor ABO-type synthases in
blood increase once accommodation is established after transplantation
and are then maintained. As their enzymatic activity decreases once rejection
occurs and recovers after treatment for rejection, it was suggested that
these enzymes can be a marker for accommodation (Fig 2).
[Photographs]
Fig1
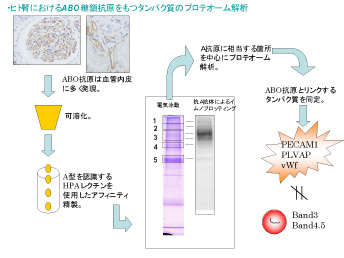
Fig2
[Area] Urologic oncology
[Research subject]
Mechanism of androgen signals in prostate cancer cells
[Description]
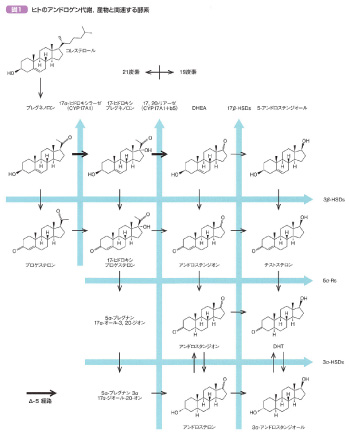
Androgen and androgen receptor are involved in the proliferation of prostate
cancer. A large amount of DHEA-S is present in human blood, and testosterone
(TT) and dihydrotestosterone (DHT) can be synthesized through various androgen
synthases in the prostate. Serum TT significantly decreases with androgen
deprivation treatment (ADT), but 25% of prostate DHT as compared to pre-ADT
remains, creating a large difference from blood concentrations [1]. In
highly malignant prostate cancer with a Gleason Score of 7 or more, prostate
DHT is lower with smaller changes before and after ADT and is less likely
to be affected by changes in blood TT [2]. Post-ADT prostate DHT concentrations
correlate with serum DHEA-S, TT, and ACTH, and it is believed that the
pituitary-adrenal endocrine axis plays a central role in the modulation
of androgen synthesis in the ADT environment [3].
[1] http://www.ncbi.nlm.nih.gov/pubmed/15534082
[2] http://www.ncbi.nlm.nih.gov/pubmed/17698092
[3] http://www.ncbi.nlm.nih.gov/pubmed/20884032
[Photographs]
Please see the Urology website for a detailed description of our research.