2025年1月17日 抗インフルエンザ剤感受性低下株調査の結果
2024-2025年シーズンの日本におけるインフルエンザ流行株と抗インフルエンザ薬感受性低下株調査の概要(2025年1月17日時点)
2024年10月から2025年1月17日までの期間にわたり、日本各地でのインフルエンザ流行状況および薬剤耐性変異を持つインフルエンザウイルスの発生状況を調査しました。本調査では、バロキサビルに対する感受性が低下するPA遺伝子の変異、およびオセルタミビルを含むノイラミニダーゼ阻害剤に対する感受性が低下するNA遺伝子の変異を検出しました。
全国7道府県の外来医療機関が本研究に協力しました。発熱、咳、喉の痛み、だるさなど、インフルエンザが疑われる症状(インフルエンザ様疾患、ILI)がある患者のうち、迅速診断テスト(RDT)でインフルエンザA型またはB型陽性と判定された方から、上気道検体を採取し、これを初診時のサンプルとしました。また、バロキサビルを投与された患者には、3~6日後に再診をお願いし、その際に再診時の上気道検体を採取しました。これらの検体はすべて新潟大学に送付され、RT-PCR法を用いてインフルエンザウイルスの検出、型/亜型の判定、PA変異およびNA変異の検出を、RT-PCR、サンガー法、次世代シーケンシング(NGS)を用いて行いました。
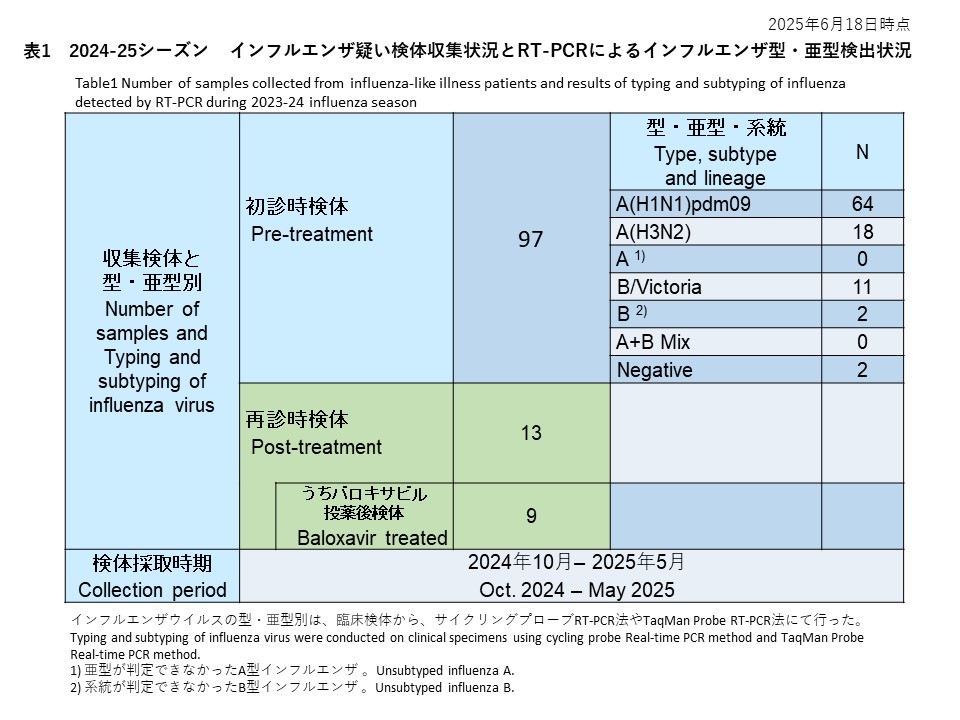
初診時に採取された29件の検体の内訳は、インフルエンザウイルスA(H1N1)pdm09が26件(89.7%)、インフルエンザウイルスA(H3N2)が1件(3.4%)、亜型判定不能のA型インフルエンザウイルスは0件(0.0%)、インフルエンザウイルスB/Victoriaが1件(3.4%)でした。また、A型およびB型の混合感染は0件(0.0%)、RT-PCR陰性の検体は1件(3.4%)でした(表1)。

サイクリングプローブRT-PCR法を用いて、治療前に採取されたインフルエンザA型の検体から、PA/I38T変異の検出を試みた結果、26件のA(H1N1)pdm09と1件のA(H3N2)のいずれからもPA/I38T変異は確認されませんでした(検出率:0%)(表2-1)。
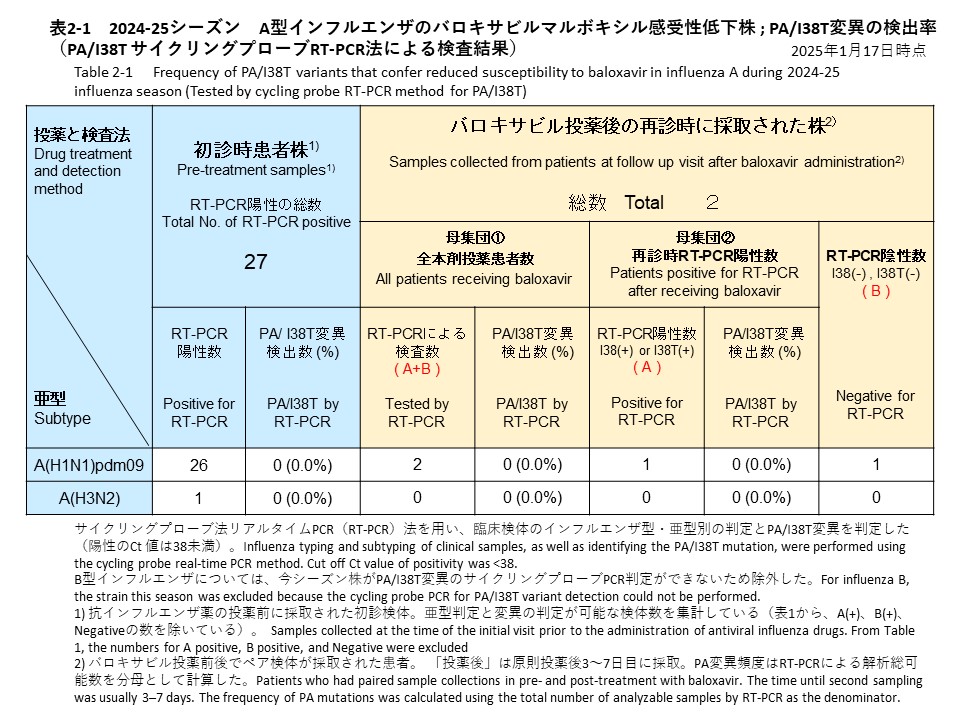
バロキサビル治療を受けた患者のうち2名(A(H1N1)pdm09が2名、A(H3N2)は0名)は、治療後3~6日目に再診した際、上気道検体を提供いただくことができました。再診時に採取した検体について、サイクリングプローブRT-PCR法を用いてPA/I38T変異を調べた結果、いずれの検体からもPA/I38T変異は検出されませんでした(検出率:0%)。検査結果の内訳は、1件がPA/I38T変異無し(感受性株)、1件がPCR陰性でした(表2-1)。
なお、サンガー法を用いたPA遺伝子の変異検出や、NGS法によるPA遺伝子およびNA遺伝子の変異解析については、現時点ではまだ実施されていません。
Overview of Influenza Circulating Strains and Antiviral Drug-Resistant Strains in Japan During the 2024-2025 Season (as of January 17, 2025)
Between October 2024 and January 17, 2025, we conducted a study across Japan to monitor influenza activity and the emergence of influenza virus strains with drug-resistant substitutions. This investigation focused on detecting substitutions in the PA gene, which reduces sensitivity to baloxavir, and substitutions in the NA gene, which reduces sensitivity to neuraminidase inhibitors, including oseltamivir. Analyses were performed using RT-PCR, Sanger sequencing, and next-generation sequencing (NGS).
Participating Medical Institutions and Sample Collection
Outpatient medical institutions in seven prefectures participated in this study. Upper respiratory tract samples were collected as initial samples from patients who visited these institutions with suspected influenza symptoms (influenza-like illness, ILI), such as fever, cough, sore throat, and fatigue. These patients were confirmed positive for influenza A or B using rapid diagnostic tests (RDTs). For patients treated with baloxavir, upper respiratory tract samples were also collected during follow-up visits 3–6 days after treatment. All clinical specimens were sent to Niigata University to detect influenza viruses, subtype determination, and detect PA and NA substitutions using RT-PCR, Sanger sequencing, and NGS.
Summary of Pre-treatment Sample Results
Among 29 samples collected during the initial visit, the results were as follows (Table 1):
A(H1N1)pdm09: 26 samples (89.7%)
A(H3N2): 1 sample (3.4%)
Unsubtyped influenza A: 0 samples (0.0%)
B/Victoria: 1 sample (3.4%)
Mixed A and B infections: 0 samples (0.0%)
RT-PCR negative: 1 sample (3.4%)
Detection of PA/I38T Substitution in Pre-Treatment Samples
Cycling probe RT-PCR detected the PA/I38T substitution in influenza A pre-treatment samples. The substitution was not detected in any of the 26 A(H1N1)pdm09 or the one A(H3N2) sample analyzed (PA/I38T detection rate: 0%, Table 2-1).
Follow-Up Samples After Baloxavir Treatment
Among patients treated with baloxavir, two individuals infected with A(H1N1)pdm09 returned for follow-up 3–6 days after treatment and provided upper respiratory tract samples. Cycling probe RT-PCR revealed no PA/I38T substitutions in either sample (PA/I38T detection rate: 0%). The results included one sample without the PA/I38T substitution (susceptible strain) and one PCR-negative sample (Table 2-1).
Pending Analyses
PA gene substitution detection using Sanger sequencing and PA/NA substitution analysis using NGS has not yet been conducted.